Published on
Differential Diagnosis
- First-degree atrioventricular block
- Left bundle branch block
- Normal sinus rhythm
- Second-degree atrioventricular block, Mobitz type I (Wenckebach)
- Second-degree atrioventricular block, Mobitz type II
Diagnosis
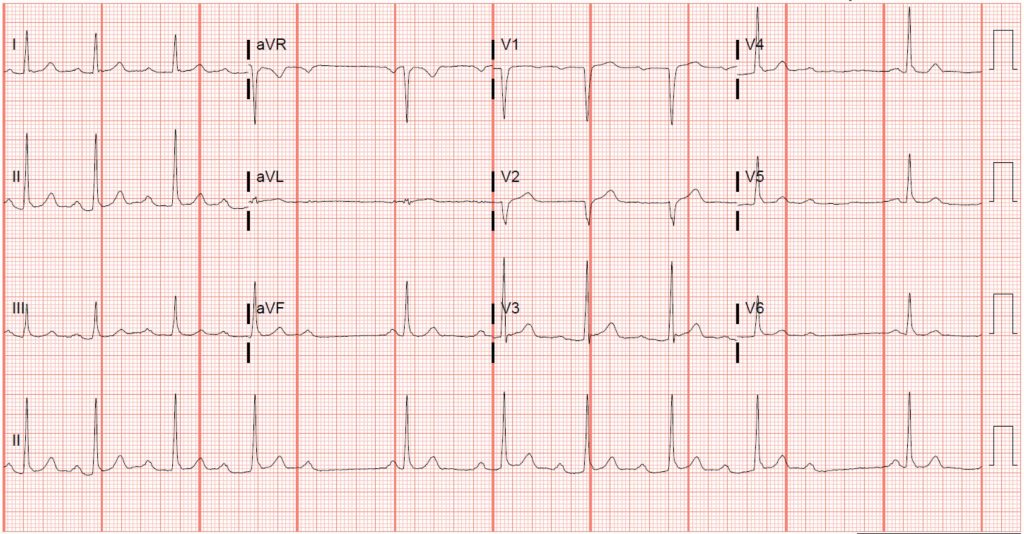
The ECG reveals a second-degree atrioventricular block, Mobitz type I (Wenckebach).
ECG Analysis
This ECG shows a ventricular rate of 60 BPM, but careful examination reveals an atrial rate of 72 BPM. The presence of more p waves than QRS complexes should prompt consideration of an atrioventricular block. In this case, p waves precede most QRS complexes, but the PR interval progressively prolongs until a QRS complex is “dropped.”
Atrioventricular conduction block refers to a set of disturbances in which conduction from the atria to the ventricles is delayed, intermittently blocked, or completely blocked—classified as first-degree, second-degree, or third-degree block, respectively.1 Identifying the type of block has important prognostic implications (Figure 1).
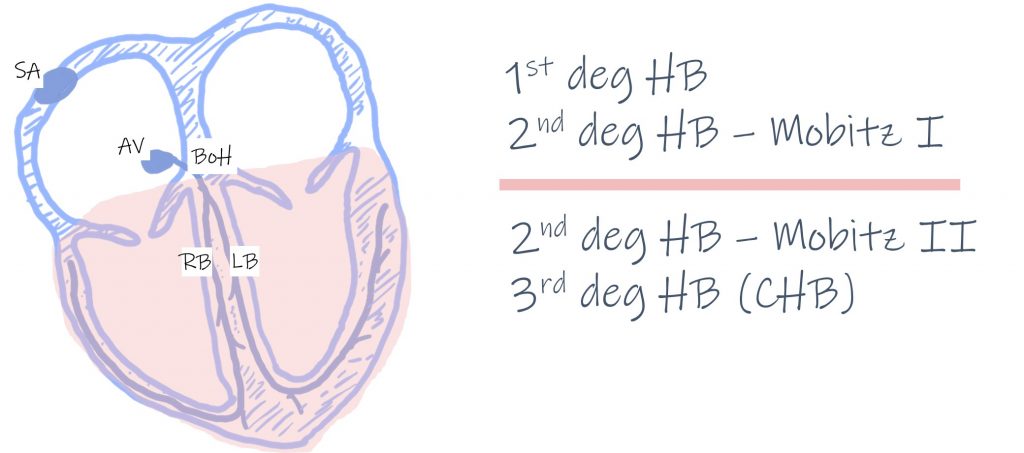
Figure 1. Conduction defects above the pink line are typically the result of delayed or intermittent conduction through the atrioventricular node; those below the pink line are the result of conduction disease below the atrioventricular node and carry a worse prognosis. (SA, sinoatrial node; AV, atrioventricular node; BoH, bundle of His; LB, left bundle; RB, right bundle; HB, heart block; CHB, complete heart block)
First-degree atrioventricular block is represented by prolongation of the atrioventricular conduction time (PR interval) beyond 0.2 s, while every atrial impulse is conducted to the ventricle. First-degree block usually suggests delayed conduction through the atrioventricular node, and is generally considered to be a benign phenomenon when not associated with other conduction deficits (ie, right bundle branch block with a concomitant left anterior or posterior fascicular block, a so-called “bifascicular block”).1,2
Third-degree atrioventricular block occurs when there is complete atrioventricular dissociation (ie, failure of conduction between the atria and the ventricles). In third-degree block, the level of escape rhythm determines not only the heart rate, but also the reliability of the rhythm. For example, when the atrioventricular node is diseased and fails to conduct, a junctional escape rhythm (at the level of the bundle of His) emerges, usually producing a more reliable rate between 40 and 60 BPM. However, when infra-Hisian conduction disease exists (ie, below the bundle of His), the escape rhythms are ventricular in origin and tend to be slower and less reliable.3 Patients with third-degree block should be immediately referred to an emergency department. Second-degree atrioventricular block occurs when there is intermittent atrioventricular conduction and can represent conduction deficits at the level of the atrioventricular node or at the infra-Hisian level. Electrocardiographically, it is characterized by a progressively prolonging PR interval until conduction from the atria to the ventricle fails (Figure 2). Second-degree Mobitz type I blocks are often asymptomatic and seen in active, healthy patients without heart disease—and usually represents disease within the atrioventricular node itself, which is unlikely to progress to complete heart block.3 Immediate referral to an emergency department is not necessary in patients with second-degree Mobitz type I block not accompanied by bundle branch block or symptoms to suggest bradycardia (eg, syncope or presyncopal lightheadedness). However, Mobitz type I block can indicate infra-Hisian conduction disease when accompanied by preexisting conduction disease (eg, right bundle branch block, left bundle branch block, or bifascicular block). Immediate referral to an ED is warranted when patients present with symptoms suggesting intermittent bradycardia.

Figure 2. Dashes represent the progressively prolonging PR interval until a ventricular beat is “dropped” (asterisk), characteristic of second degree atrioventricular block, Mobitz type I.
Second-degree atrioventricular block, Mobitz type II almost always occurs when there is infra-Hisian conduction disease and is characterized electrocardiographically by a constant PR interval with dropped beats (Figure 3). Patients with this rhythm should be immediately referred to the ED for consideration of a permanent pacemaker, since this conduction deficit is likely to progress to complete heart block.3
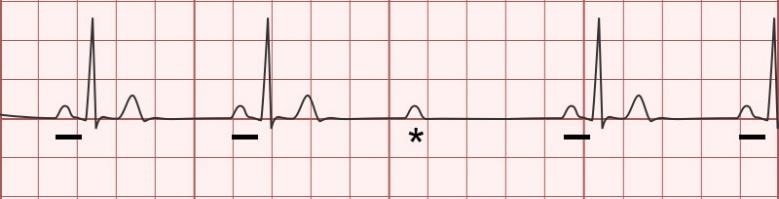
Figure 3. Second-degree atrioventricular block, Mobitz type II. Dashes represent a constant PR interval; a ventricular beat is “dropped” (asterisk), characteristic Image adapted with permission from ddxof.com.
Learnings/What to Look for:
- The presence of more p waves than QRS complexes should prompt consideration of an atrioventricular block
- The recognition between Mobitz I and II is important, as there are prognostic implications
- First-degree atrioventricular block and second-degree Mobitz type I block generally represent delayed conduction through the atrioventricular node and are not likely to progress to complete heart block
- Second-degree Mobitz type II block and third-degree block (ie, complete heart block) represent infra-Hisian conduction disease and warrant emergent consideration
Pearls for initial management and considerations for transfer:
- Patients with atrioventricular blocks thought to represent infra-Hisian disease should be immediately referred to an ED
- Patients with atrioventricular blocks thought to represent atrioventricular nodal conduction delay do not need immediate referral to an ED
- In patients with unstable bradycardia secondary to atrioventricular block, consider transcutaneous pacing and immediate referral to the emergency department
References
1. Costa D Da, Brady WJ, Edhouse J. Bradycardias and atrioventricular conduction block. Br Med J. 2002;324(March):535-538.
2. de Pádua F, Pereirinha A, Marques N, et al. In: Macfarlane PW, van Oosterom A, Pahlm O, Kligfield P, et al, eds. Comprehensive Electrocardiology. London: Springer London; 2010:547-604.
3. Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm. Circulation. 2019;140(8):e382-e482.